|
|
The Impossibility of the 14cm Acromion Autopsy Measurement
Chad R. Zimmerman © Copyright 2004. All Rights Reserved.
|
|
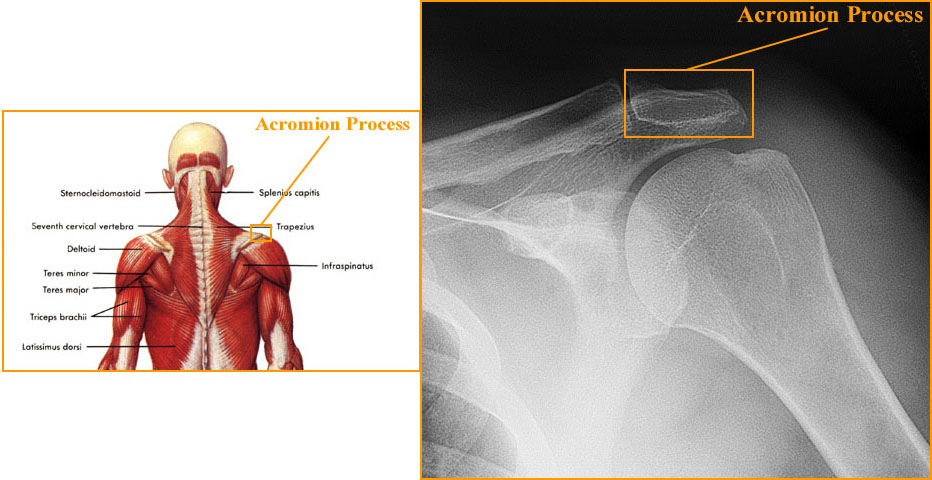
Since the autopsy findings became public information, our public has scrutinized the pathologists' findings with a fine toothed comb. One of the perplexing issues surrounds the anatomical location of President Kennedy's initial wound to the upper back, or lower neck. In the final autopsy report, Dr. Humes specified the location of the wound by measuring from two anatomical reference points. While he should've used fixed body landmarks, such as the spine, he used the right 'mastoid process' and the right 'acromion process'. The mastoid process is a prominence of the temporal bone and lies just behind the external ear canal. For reference regarding the acromion process, please see the anatomical illustration below.
|
|
|
|
As seen above, the acromion process is a named prominence on the scapula, or shoulder blade. This process creates the tip of the shoulder. The average person, while in an anatomically neutral position, has their acromion process in a horizontal line with the T1-2 vertebral level. That is, even with the first or second thoracic vertebra. The acromion process is not a fixed anatomical landmark, therefore it moves in different anatomical positions. Because of this movement, it is not an ideal point on the body to measure bullet wounds from. The Bethesda autopsists should've measured from the spine instead, since that is considered a fixed body landmark. Measurements from fixed body landmarks are easily correlated and reproducible. If measured from a movable body landmark, the measurement can change and errors occur in reproduction. This is what has occurred as a result of the Bethesda autopsists measuring from the acromion. They obtained a measurement of 140mm, or 14cm, from the right acromion process. This wound was also noted to be 1-2 inches from the spine.
Many astute researchers have examined this and found it to be impossible. Apparently, the distance is too narrow to have a 14cm measurement from the right acromion to a point 1-2 inches from the spine. In fact, one researcher even attempted to obtain a close measurement on her adolescent son and obtained 17cm....or just shy of 2 inches too long. So, why does it even matter? If the measurement is impossible, then the autopsists lied or failed to measure. Why would they do that? Conspiracy, of course! This usually leads to the conclusion that President Kennedy was actually hit much lower in the spine than the autopsy report indicated and that the autopsists needed to falsify a location that allowed for a downward, rear trajectory for the lone gunman- Lee Harvey Oswald.
|
|
The Veracity of the Claim- Putting it to the Test
I decided to put this claim to the test, using reproducible scientific technique. I had studied this issue quite extensively and found several basic flaws. First of all, several witnesses noted that the wound appeared to be below the level of the shoulder tip (acromion). This would put it at the level of about T3. However, after looking at the autopsy photographs and correlating them to the x-rays, one crucial point of interest develops. President Kennedy was not in a neutral position at the time of autopsy. His shoulders were elevated to the point that his clavicle attained the level of C5-6, instead of the anatomically neutral level of T1. Hence, his body position was not anatomically neutral, but most researchers are measuring their subjects in a neutral, or very near neutral position. So, in essence, most researchers are trying obtain 'like' results in a very un-'like' manner. Naturally, the results will most likely differ.
Linear Distance
I decided to test the theory as completely as possible. First, I decided to take an AP thoracic x-ray to determine the linear distance from my spine to my acromion process. This should be simple elimination, right? If the measurement is way off, then it's impossible and I can move on, knowing that the autopsists falsified information and a possible conspiracy was afoot. So, I took the x-ray and measured. See below:
|
|
(Sorry, I'll get to this soon)
|
|
In the above x-ray, several measurements can be made. Since nobody knows exactly where on the acromion Humes measured from, I ascertained it's position from the spine with several measurements. First, I measured the distance from the medial (towards the middle, or midline) acromion to opposite medial acromion. This measured 364mm, or 36.4cm. Next, I measured from the lateral (away from the middle, or midline) to the opposite lateral acromion. This measured 420mm, or 42cm. (Since one acromion was out of the x-ray frame, I assumed symmetry between both sides.) Lastly, I measured from the center of the spine to both the medial and lateral aspects of the right acromion process. The lateral measured 21.5cm and the medial edge was 18.7cm from the center of the spine. So, this gave me an estimated range of 18.7cm-21.5cm from the center of the spine to my right acromion process, depending on where on the acromion I would measure to. Looking at the full distance between acromion processes, it becomes apparent that my right acromion is slightly further from my spine than the left. This may be due to anatomical asymmetry, considered a normal variant, or positional error during the x-ray evaluation. However, the assumed error would be very slight.
In effect, on x-ray, my acromion lies in an area 7.36"-8.46" from the center of my spine. Since the wound on Kennedy has been estimated at 1-2" (2.54-5.08cm) right of the spine, we can use my x-ray as a guide to the feasibility of the measurement. If you subtract 1-2" from my measurements, the similar wound to me would lie in a range between 5.36"-6.46" from my spine. 14cm equals 5.51". It appears that, at least on me, it works. However, it barely meets the requirement, until you look a bit further.
X-rays cause magnification. Since x-rays travel in a straight line and are emitted from a narrow source over a wider area, the resulting image is distorted through magnification. The actual linear distance from my spine to my acromion is less than that seen on x-ray. So, I needed to figure out how much magnification may have resulted on my x-ray. In order to do so, I needed to know about how far my acromion was from the film. So, I stood in the same position that I had been when the x-ray was taken and measured the distance from my back to the film bucky (the device that holds the film cassette). While standing, we approximated the distance from the bucky using a metric ruler. The posterior acromion to bucky distance was approximately 7cm, while the anterior acromion to bucky distance was approximately 13cm. In order to ascertain the magnification, I took a metal object of known dimension (penny) and x-rayed it twice, once 7cm and once 13cm from the film bucky. The width of the penny is exactly .75", or 19.05mm (1.905cm).
Setup:
I positioned myself in front of the x-ray bucky as I did for my x-ray. I then marked the film bucky behind my right acromion process. I took a paper towel roll and cut two short slits in it at 7cm and 13cm. I attached the paper towel roll to the film bucky and placed the penny in one of the two slits and took the film. The x-ray was repeated at the other slit. The x-ray tube to film distance remained constant for all films. The films were developed and the width of the corresponding penny 'opacity' was measured using both a metric ruler and a micrometer for comparison purposes.
Measurement Results:
The width of the penny at 7cm was measured to be 20.5mm by ruler and 20.6mm by micrometer for an average of 20.55mm, or .809". The width of the penny at 13cm was measured to be 21.6mm by ruler and 21.5mm by micrometer for an average of 21.55mm, or .848". This gives us a good range to calculate the probable magnification that affected the measurements in my x-ray.
Since the known width of the penny was .75", or 19.05mm, the magnification increase can be calculated.
(Film width - Known width)
____________________=
Known width
Using the above formula and the average widths of the penny on x-ray, I calculated the percentage increase to be:
At 7cm, the percentage increase equals 7.87%
At 13cm, the percentage increase equals 13.12%
Anatomy:
The average acromion process has it's most medial point anteriorly and the most lateral portion posteriorly. So, less distortion would be present at the lateral portion, but more on the medial on an AP x-ray. However, since I cannot know the exact percentage increase, I'll compute a range based on the above percentages. In addition, there is less distortion towards the center of the film. In other words, the distortion increases the futher you get from the central ray of the x-ray machine. For example, I took the same paper towel roll and penny and refilmed with the central ray over the penny. The distortion was noticeably less, yet still significant.
Central Ray Penny Results (i.e. minimum magnification):
At 7cm, the width of the penny on x-ray was measured with a metric ruler to be 20.2mm, or .798", and 20.21mm, or .796", by micrometer.
At 13cm, the width of the penny on x-ray was measured with a metric ruler to be 21mm, or .827", and 20.67mm, or .814", by micrometer.
Average:
7cm with central ray- .797" or 20.24mm
13cm with central ray- .821" or 20.85mm
Percentage Increase:
Using the same formula above, I computed the percentage increase to be the following:
At 7cm, the percentage increase equals 6.27%.
At 13cm, the percentage increase equals 9.47%
Conclusion:
Even minimizing the magnetic distortion through positioning with the central ray, I still found a minimum magnification of 6.27%. Therefore, the minimum magnification of my spinal x-ray would be 6.27%, with a possible range up to 13.12%. This may not be the actual uppermost degree of magnification; yet I believe it to be close with respect to the x-ray in question. My shoulder would have to be further lateral in order to increase the magnification. Care was taken to ensure similar positioning and I believe any error to be minimal.
Since I have established a working degree of magnification, I can now calculate a range of linear distances from my spine, a mock wound such as JFK's to the acromion process; both lateral and medial. Now, the spine to medial acromion measured 18.7cm with magnification. Now, using algebra, we can compute the range for the maximum linear distance, instead of x-ray distance. The linear equation is thus:
106.27x = 18700mm
x = 175.97mm, or 17.6cm
Since this is the minimum percentage increase, it represents the largest actual linear distance. Now, let's look at the other end of the percentile increase range based on the maximum percentage increase noted above.
113.12x = 18700mm
x = 165.31mm, or 16. 5cm
Therefore, the actual distance, depending on x-ray magnification equals between 16.5cm and 17.6cm, or 6.49" - 6.92", from the center of the spine to the medial aspect of the acromion process depending on the degree of magnification. Using our established numbers above for a wound 1-2" right of the spine, we can compute an actual linear range of:
4.49"(with wound 2" from spine) - 5.92" (with wound 1" from spine)
Kennedy's wound was measured to be 14cm, or 5.51", from the acromion and estimated at 1-2" right of the spine. When magnification is taken into account, one can conclude that it is very possible to have a linear distance of 14cm with the above criteria. Errors occur in many areas when researchers try to measure on live human subjects. They involve:
1. Measuring the contour of the back instead of the linear distance. This increases the total distance.
2. Improper body position.
3. Remedial understanding of human anatomy; leads to inaccurate placement of the acromion.
4. Improper body type; subjects with broad shoulders would be expected to have larger measurements. Kennedy was not a large, or broad shouldered man. He was 6'0" tall and 170lbs. at the time of autopsy.
For a very good look at the other 'side' of the issue, Barb Junkkarinen put a good article together that can be found here: http://www.jfklancer.com/pdf/barbj.pdf
|